General Information About Salivary Gland Cancer
- Salivary gland cancer arises in the tissues of the salivary glands.
- Being exposed to radiation may increase the risk of salivary cancer.
- Salivary gland cancer usually presents with a lump
Salivary gland cancer is a rare disease in which cancer cells arise form in the tissues of the salivary glands.
The salivary glands make saliva and release it into the mouth. There are 3 pairs of major salivary glands:
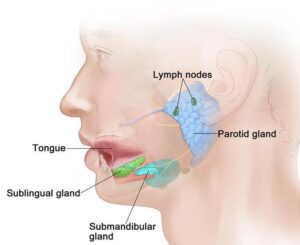
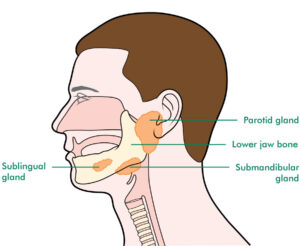
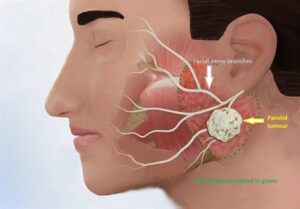
- Parotid glands: These are the largest salivary glands and are found in front of and just below each ear.
- Sublingual glands: These glands are found under the tongue in the floor of the mouth.
- Submandibular glands: These glands are found below the jawbone.
There are also hundreds of small (minor) salivary glands lining parts of the mouth, nose, and larynx that can be seen only with a microscope. Most minor salivary gland tumours begin in the palate (roof of the mouth). The majority of the salivary gland tumours are benign (not cancerous) and do not spread to other tissues.
Being exposed to radiation may increase the risk of salivary cancer.
The cause of most salivary gland cancers is not known. Risk factors include the following:
- Older age.
- Treatment with radiation therapyto the head and neck.
- Harbouring a specific benign salivary gland tumour called pleomorphic adenoma (PSA) for many years.
Salivary gland cancer usually presents with a lump.
Salivary gland cancer is usually asymptomatic. It may be found during a regular dental check-up or physical exam. Check with your doctor if you have any of the following:
- A lump (usually painless) in the area of the ear, cheek, jaw, lip, or inside the mouth.
- Trouble in opening the mouth widely.
- Numbness or weakness in the face.
- Pain in the face that does not go away.
Examination, diagnosis, investigations (Need Photos)
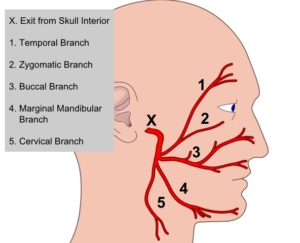
- Clinical examination and history: Your OMFS H&N surgeon will ask about your social habits (smoking and drinking) and take a thorough medical history. The neck will be felt for swollenlymph nodes. He will feel any lumps related to the salivary glands. He will examine the function of your facial nerve F8 (the nerve that helps you move your face and is responsible for your facial expression), He will do that by asking you to raise your eyebrows, whistle, close your eyes tightly and puff up your cheeks.
- Biopsy:This is paramount in order to diagnose cancer. Your OMFS H&N Surgeon will take a sample of the abnormal area.
- Fine Needle Aspiration: This is a form of biopsy, but instead of tissue sample, the OMFS H&N Surgeon samples few cells with the help of a syringe and needle. This is usually the case for lumps related to the salivary glands. The cells are viewed under a microscope to find out if they are abnormal.
- Core biopsy: This is similar to the FNA, but instead of a needle, a biopsy gun is used, that takes more tissue and allows for more confident histological diagnosis.
- MRI (Magnetic Resonance Imaging): A procedure that uses a magnet, radio waves, and a computer to make a series of detailed pictures of areas inside the body. An MRI of your H&N region is required to stage the cancer

- CT scan: A computerised x-ray that makes a series of detailed pictures of areas inside the body, taken from different angles. A CT scan of your thorax (chest) is needed for staging H&N cancer, to exclude disease spread and/or second primaries in the lung.
Factors affecting the outcome
The prognosis (chance of cure and recovery) depends on:
- The fitness of the patient
- Whether the patient is/was a smoker.
- The stageof the cancer.
- The type of the cancer (how does it look under the microscope)
- The location of the cancer.
Stages of salivary gland Cancer
- There are three ways that cancer spreads in the body.
- Cancer may spread from where it began to other parts of the body.
- The following stages are used for laryngeal cancer:
- Stage 0 (Carcinoma in Situ)
- Stage I
- Stage II
- Stage III
- Stage IV
The way salivary gland cancer is staged is complex – your OMFS H&N surgeon will explain the stage and the implications once all tests are completed.
The process used to find out if salivary gland cancer has spread to other parts of the body is called staging. Staging guides decision-making and treatment.
There are three main ways that cancer spreads in the body.
Cancer can spread through tissue, the lymph system, and the blood:
- The cancer spreads from where it began by growing into nearby areas. Some types of salivary gland cancer prefer to spread across nerves (perineural spread)
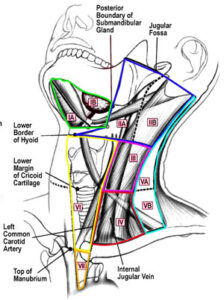
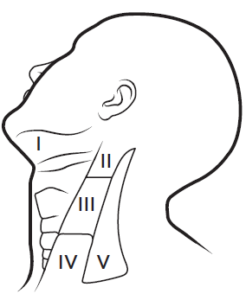
- Lymph system. The cancer spreads to the lymph glands (in H&N cancer it spreads in the neck lymph glands).
- The cancer spreads from where it began by getting into the blood. The cancer travels through theblood vessels to other parts of the body (distant metastasis).
When cancer spreads to another part of the body, it is called metastasis.
Treatment
- The primary treatment for salivary gland cancer is surgery
- Minor salivary gland tumours in the oral cavity are treated the same way as any other mouth cancer (see chapter)
- Radiotherapy is used as adjuvant treatment after surgery in selected cases
- Patients with salivary gland cancer should have their treatment planned and delivered by a team who is expert in treating head and neck cancer.
- Two types of standard treatment are used:
- Surgery(primary treatment)
- Radiation therapy (adjuvant)
- Treatment for salivary gland cancer is difficult, complex and may cause side effects.
- Follow-up tests may be needed.
Patients with salivary gland cancer should have their treatment planned by a team of doctors who are expert in treating head and neck cancer.
Your expert OMFS/H&N Surgeon, who will guide the team for you, will oversee your treatment. A team approach is required to overcome the potential side effects of the treatment. The team usually include:
- Head and necksurgeon (ablation and reconstruction)
- Radiation oncologist
- Speech therapist
- Dietitian
- Pathologist
- Radiologist
- CNS
Surgery
Surgery (removing the cancer in an operation) is the first line treatment for salivary gland cancer. Surgery might include the following:
- Parotidectomy (Superficial, Total, Radical): This procedure removes the cancer from the parotid salivary gland, alongside with healthy salivary gland tissue. Depending of the extend of the tumour, the surgeon might remove the superficial part of the parotid gland (superficial parotidectomy), all of the parotid gland (total parotidectomy) or all the parotid gland and surrounding structures (radical parotidectomy). Every effort is made to preserve the facial nerve that runs within the substance of the parotid salivary gland. Occasionally, removing the nerve is needed to get clearance of the cancer, and on these occasions, cable nerve grafting with microsurgery is needed.


- Neck dissection: Removal oflymph nodes in the neck. This is done when cancer has or may have spread from the salivary glands. This also provides access to blood vessels for microvascular reconstruction.
- Reconstruction: In cases that the resection of the salivary gland cancer includes surrounding structures (skin, bone, oral cavity mucosa) your OMFS Surgeon will discuss reconstruction options with you. This is a highly demanding and highly important part of your cancer treatment. The defect created by the removal of the tumour needs to be re-build to improve function and reduce the risk of potential side effects. The gold standard is the use of microvascular free tissue transfer (the surgeon takes tissue – skin, muscle, bone or combinations – from other parts of the patients’ body, preserving the blood vessels and re-perfuse the flap by anastomosing the blood vessels with donor vessels in the neck. This is called microvascular surgery and it is done under the operating microscope. Cable nerve grafting is another form of microsurgery. Offering this kind of treatment should be the minimum you would expect from your OMFS H&N Surgeon.
Radiatiotherapy
Radiatiotherapy is a cancer treatment that uses high-energy radiation to kill cancer cells or keep them from growing. For salivary gland cancers, it is often used as adjuvant therapy. Unlike other forms of head and neck cancer, chemotherapy doesn’t seem to have an effect and is rarely used
Side Effects
Treatment for salivary gland cancer is difficult and can result in life-changing side effects. Your OMFS H&N surgeon will follow you up and try to deal with these side effects whenever possible
- Xerostomia – dry mouth
- Difficulties in speech
- Difficulties in swallowing (may require feeding tube)
- Changes in appearance
- Weight loss
- Infection
- Lymphedema
- Chronic pain
- Osteoradionecrosis (ORN)
- Shoulder dysfunction
- Taste changes
- Scarring
- Facial nerve weakness