General Information About Neck Unknown Primary Cancer
- Neck unknown cancer is a disease found in the neck lymph nodes and it is not known where the cancer has started.
- Signs and symptoms include a painless neck lump.
- Tests are needed to confirm that the neck lump is cancerous and to try to identify the primary tumour.
Neck unknown cancer is a disease found in the neck lymph nodes and it is not known where the cancer has started
Cancer can begin in cells anywhere in the body and metastasize (spread) through the blood or lymph system to other parts of the body. When squamous cell cancer spreads to lymph nodes in the neck or around the collarbone, it is called metastatic squamous neck cancer. Your OMFS H&N Surgeon will exhaust all efforts to find the primary tumour (the cancer that first formed in the body), because that will determine the appropriate treatment. Occasionally, the primary cancer cannot be found. In that case, it is called an occult (hidden) primary tumour. In many cases, the primary tumour is never found.
Signs and symptoms
See your OMFS H&N surgeon for any lump in the neck. The risk is increased if you are over 40 and the lump persists or you have earache/neck pain.


Examination, diagnosis, investigations
- Clinical examination and history: Your OMFS H&N surgeon will ask about your social habits (smoking and drinking) and take a thorough medical history. He will thoroughly examine your mouth, your throat, the skin of your face and scalp, and feel your neck for swollenlymph nodes.
- Fiberoptic nasoendoscopy: This examination is of paramount importance. Your OMFS H&N surgeon will pass a thin tube-like camera through your nose, to examine the back of your throat, the base of your tongue and your voice box (larynx).
- Fine Needle Aspiration: This is a form of biopsy, but instead of tissue sample, the OMFS H&N Surgeon samples few cells with the help of a syringe and needle. This is usually the case for lumps in the neck (lymph nodes). The cells are viewed under a microscope to find out if they are abnormal.
- MRI (Magnetic Resonance Imaging): A procedure that uses a magnet, radio waves, and a computer to make a series of detailed pictures of areas inside the body. An MRI of your H&N region is required as a first line attempt to identify the hidden primary cancer

- CT scan F5: A computerised x-ray that makes a series of detailed pictures of areas inside the body, taken from different angles. A CT scan of your thorax (chest) is needed for staging H&N cancer, to exclude disease spread and/or second primaries in the lung. In the case of unknown primary cancer, this might show the hidden lesion in other parts of the body (i.e. lungs)

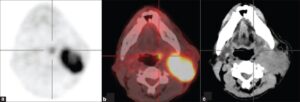
- PET scan (positron emission tomography scan): This is the gold standard investigation for cancer of unknown primary. It is a procedure that aims to find malignant tumourcells in the body. A small amount of radioactive glucose (sugar) is injected into a vein. The PET scanner takes picture of where glucose is being used in the body. Malignant tumour cells show up brighter in the picture because they are more active and take up more glucose than normal cells do. The PET scan is particularly useful when the cancer present as an isolated neck lump and the primary tumour is very small (usually hidden in the base of the tongue or the tonsils).
- EUA (Examination Under Anaesthesia): For this exam, you will be asleep. Your OMFS H&N surgeon will thoroughly examine the areas of your throat and take samples from abnormal looking areas. Occasionally (especially in cases of neck occult primary) your surgeon might need to sample areas of your tongue base and remove your tonsils, even if they look normal, as the primary cancer might be very small and indolent.
- Epstein-Barr virus(EBV) and human papillomavirus (HPV) test: A test that checks the cells in a sample of tissue for EBV and HPV DNA. This is important, as the majority of the neck unknown primary tumours originate from the oropharynx (and most are HPV related) or the nasopharynx (and most are EBV related)
Factors affecting the outcome
The prognosis (chance of cure and recovery) depends on:
- Whether the cancer is HPV related
- Whether the patient is/was a smoker
- The stageof the cancer
- Whether the primary tumour is found or not
Treatment options depend on the following:
- The stage of the cancer.
- Whether the occult primary is more likely to originate from the H&N area
- The patient’s general health.
Stages of neck occult primary
- If the primary tumour isn’t identified despite extensive tests, then the T-stage is T0
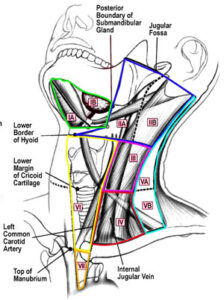
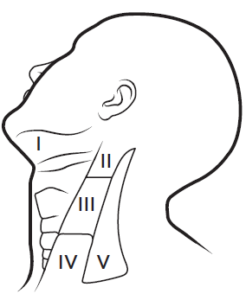
- The N-stage (indicating spread to the neck lymph nodes) is done as per any other H&N cancer
There are three main ways that cancer spreads in the body.
Cancer can spread through tissue, the lymph system, and the blood:
- The cancer spreads from where it began by growing into nearby areas.
- Lymph system. The cancer spreads to the lymph glands (in H&N cancer it spreads in the neck lymph glands). This is the way that most of the times a very small or non-identified primary (occult) is spread in the neck, in case of neck unknown primary cancer.
- The cancer spreads from where it began by getting into the blood. The cancer travels through theblood vessels to other parts of the body (distant metastasis).
When cancer spreads to another part of the body, it is called metastasis.
Treatment
- If the primary tumour is found, then treatment follows the principles of treatment of that location
- If the primary remains occult, then treatment is given to the neck and occasionally to the areas that are most likely to harbour the unknown primary (i.e. oropharynx, especially in cases of HPV-related neck disease)
- A neck dissection (selective removal of the neck lymph glands with surgery is the first line treatment in cases of neck unknown primary
- Radiotherapy with or without chemo is used as adjuvant treatment following surgery (both to the neck and potential primary site (s))
- Treatment for unknown primary cancer is difficult, complex and may cause side effects.
- Follow-up tests may be needed.
Patients with cancer of unknown primary should have their treatment planned by a team of doctors who are expert in treating head and neck cancer.
Your expert OMFS/H&N Surgeon, who will guide the team for you, will oversee your treatment. The oropharynx (throat), neck and face are vital areas for eating, drinking, talking, cosmesis and psychology. A team approach is required to overcome the potential side effects of the treatment. The team usually include:
- Head and necksurgeon (ablation and reconstruction)
- Radiation oncologist
- Speech therapist
- Dietitian
- Pathologist
- Radiologist
- CNS
Surgery
Neck dissection: Removal of lymph nodes in the neck. This allows further characterization of the tumour, reduces the bulk of the disease and allows radiotherapy to work better at a microscopic level
Radiatiotherapy
Radiatiotherapy is a cancer treatment that uses high-energy radiation to kill cancer cells or keep them from growing. It is usually given after the surgery, depending on specific indications, and is called adjuvant therapy. Occasionally, in the event of extracapsular spread (ECS) in the neck glands, radiotherapy will be given combined with chemotherapy, to increase its efficacy. For unknown neck primary cancer, radiotherapy is also given at a reduced dose in the areas most likely to harbour the hidden primary tumour (i.e. oropharynx – tongue base and tonsils)
Side Effects
Treatment for cancer of unknown primary is difficult and can result in life-changing side effects. Your OMFS H&N surgeon will follow you up and try to deal with these side effects whenever possible
- Xerostomia – dry mouth
- Difficulties in speech
- Difficulties in swallowing (may require feeding tube)
- Changes in appearance
- Weight loss
- Infection
- Lymphedema
- Chronic pain
- Osteoradionecrosis (ORN)
- Shoulder dysfunction
- Taste changes
- Scarring