Mouth Cancer (Lip and Oral cavity)
- Lip and oral cavity cancer is a disease in which malignant (cancer) cells form in the lips or mouth.
- Most mouth cancers are caused by smoking and alcohol.
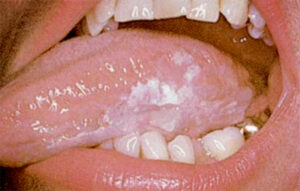
- Lip and oral cavity cancers often present with an ulcer or a lump on the lips or in the mouth. However, they can also present more indolently, in the form of an innocent looking white patch
- Clinical examination usually identifies the lesion; biopsy confirms it and scans are used to stage the disease.
- Certain factors affect prognosis (chance of cure and recovery) and treatment options.
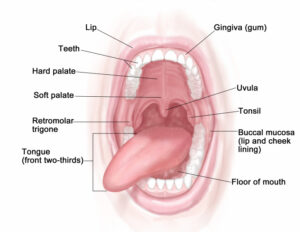
Basic Anatomy
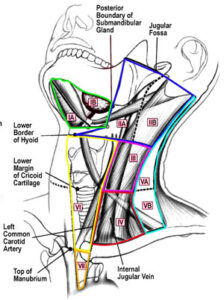
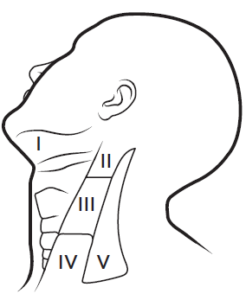
Anatomy of the neck muscles
The oral cavity includes the following:
- The front two thirds of the tongue
- The gingiva (gums)
- The buccal mucosa (the lining of the inside of the cheeks)
- The floor (bottom) of the mouth under the tongue
- The hard palate (the roof of the mouth)
- The retromolar trigone (the small area behind the wisdom teeth)
Most lip and oral cavity cancers are squamous cell carcinomas (originate from squamous cells; the thin, flat cells that line the lips and oral cavity).
Risk Factors
Anything that increases your risk of getting cancer is called a risk factor. Having a risk factor does not mean that you will get cancer; not having risk factors doesn’t mean that you will not get cancer.
- Smoking (any form; cigarettes, pipe, shisha)
- Heavy alcohol
- Chewing tobacco or betel nut (common in Asia)
- Some forms of oral lichen planus
Presentation
Early diagnosis is paramount for increasing the chances of cure. See your OMFS H&N surgeon if you have any of the following:
- An ulcer in the mouth or the lip that does not heal.


- A lump or thickening on the lips or gums or in the mouth.



- A white or red patch on the gums, tongue, or lining of the mouth.


- Bleeding, pain, or numbness in the lip or mouth
- Earache
- Change in voice
- Loose teeth or dentures that no longer fit well
- Trouble chewing or swallowing or moving the tongue or jaw
- Swelling of jaw
- Sore Throat or feeling that something is stuck in the throat
Sometimes, mouth cancer can be completely asymptomatic and found during a regular dental exam.
Examination, diagnosis, investigations
- Clinical examination of the mouth: Your OMFS H&N surgeon will ask about your social habits (smoking and drinking) and take a thorough medical history. He will exam the lips and oral cavity looking for any abnormality. Your OMFS H&N surgeon will look carefully and feel the entire mouth with a gloved finger and examine the oral cavity with a mirror and good light. The neck will be felt for swollen lymph nodes.
- Fiberoptic nasoendoscopy: If needed, your OMFS H&N surgeon will pass a thin tube-like camera through your nose, to examine the back of your throat, the base of your tongue and your voice box (larynx).
- Biopsy: This is paramount in order to diagnose cancer. Your OMFS H&N surgeon will take a sample of the abnormal area, usually under local anaesthetic, and send it to be viewed under a microscope by a pathologist.
- Fine Needle Aspiration: This is a form of biopsy, but instead of tissue sample, the OMFS H&N surgeon samples few cells with the help of a syringe and needle. This is usually the case for lumps in the neck (lymph nodes). The cells are viewed under a microscope to find out if they are abnormal.
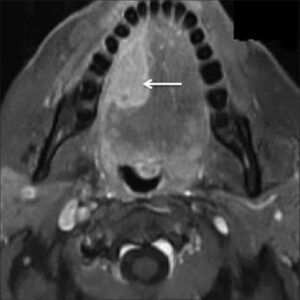
- MRI (Magnetic Resonance Imaging): A procedure that uses a magnet, radio waves, and a computer to make a series of detailed pictures of areas inside the body. An MRI of your H&N region is required to stage the cancer.

- CT scan: A computerised x-ray that makes a series of detailed pictures of areas inside the body, taken from different angles. A CT scan of your thorax (chest) is needed for staging H&N cancer, to exclude disease spread and/or second primaries in the lung.

- PET scan (positron emission tomography scan): A procedure to find malignant tumour cells in the body. A small amount of radioactive glucose (sugar) is injected into a vein. The PET scanner takes picture of where glucose is being used in the body. Malignant tumour cells show up brighter in the picture because they are more active and take up more glucose than normal cells do.
Factors affecting the outcome
Prognosis (chance of cure and recovery) depends on the following:
- The stage of the cancer
- The location of the cancer
- Whether the cancer has spread
For patients who smoke, the chance of recovery is better if they stop smoking before the beginning of treatment
Treatment options depend on the following:
- The stage of the cancer
- The size and the location of the tumour
- The patient’s general health
Patients who have had lip and oral cavity cancer have an increased risk of developing a second cancer in the head or neck, or a synchronous cancer in the lung. Frequent and careful follow-up is important.
Stages of mouth Cancer
KEY POINTS
- After mouth cancer has been diagnosed (positive biopsy), tests are done to find out if cancer cells have spread within the lip and oral cavity or to other parts of the body.
- There are three ways that cancer spreads in the body.
- Cancer may spread from where it began to other parts of the body.
- The following stages are used for lip and oral cavity cancer:
- Stage 0 (Carcinoma in Situ)
- Stage I
- Stage II
- Stage III
- Stage IV
The way mouth cancer is staged is complex – your OMFS H&N surgeon will explain the stage and the implications once all tests are completed
The process used to find out if cancer has spread within the lip and oral cavity or to other parts of the body is called staging. Staging guides decision-making and treatment.
There are three main ways that cancer spreads in the body.
Cancer can spread through tissue, the lymph system, and the blood:
- The cancer spreads from where it began by growing into nearby areas.
- Lymph system. The cancer spreads to the lymph glands (in H&N cancer it spreads in the neck lymph glands).
- The cancer spreads from where it began by getting into the blood. The cancer travels through the blood vessels to other parts of the body (distant metastasis).
When cancer spreads to another part of the body, it is called metastasis.
Treatment
- Surgery is the first and primary treatment option for mouth cancer
- Patients with mouth cancer should have their treatment planned and delivered by a team who is expert in treating head and neck cancer.
- Two types of standard treatment are used:
- Surgery (first line)
- Radiation therapy (adjuvant)
- Chemotherapy (only in selected cases and as adjunct to radiotherapy)
- Treatment for mouth cancer is difficult, complex and may cause side effects.
- Follow-up tests may be needed.
Patients with mouth cancer should have their treatment planned by a team of doctors who are expert in treating head and neck cancer.
Your expert OMFS/H&N Surgeon, who will guide the team for you, will oversee your treatment. Mouth, neck and face are vital areas for eating, drinking, talking, cosmesis and psychology. A team approach is required to overcome the potential side effects of the treatment. The team usually include:
- Head and Neck Surgeon (ablation and reconstruction)
- Radiation oncologist
- Speech therapist
- Dietitian
- Pathologist
- Radiologist
- CNS
Surgery
Surgery (removing the cancer in an operation) is the first line treatment for mouth cancer. Surgery includes the following:
- Wide local excision of the primary tumour: Removal of the cancer and some of the healthy tissue around it. If cancer has spread into bone, surgery may include removal of the involved bone tissue.
- Neck dissection: Removal of lymph nodes in the neck. This is done when cancer has or may have spread from the lip and oral cavity. This also provides access to blood vessels for microvascular reconstruction.
- Reconstruction: This is a highly demanding and highly important part of mouth cancer treatment. The defect created by the removal of the tumour needs to be re-build to improve appearance and function and reduce the risk of potential side effects. The gold standard is the use of microvascular free tissue transfer (the surgeon takes tissue – skin, muscle, bone, or combinations – from other parts of the patients’ body, preserving the blood vessels and re-perfuses the flap by anastomosing the blood vessels with donor vessels in the neck. This is called microvascular surgery and it is done under the operating microscope). Offering this kind of treatment should be the minimum you would expect from your OMFS H&N Surgeon.
Radiatiotherapy
Radiatiotherapy is a cancer treatment that uses high-energy radiation to kill cancer cells or keep them from growing. It is usually given after the surgery, depending on specific indications, and is called adjuvant therapy. Occasionally, in the event of residual tumour after surgery or if there is disease in the neck glands with extracapsular spread (ECS), radiotherapy will be given combined with chemotherapy, to increase its efficacy.
Side Effects
Treatment for mouth cancer is difficult and can result in life-changing side effects. Your OMFS H&N surgeon will follow you up and try to deal with these side effects whenever possible
- Xerostomia – dry mouth
- Difficulties in speech
- Difficulties in swallowing (may require feeding tube)
- Changes in appearance
- Weight loss
- Infection
- Lymphedema
- Chronic pain
- Osteoradionecrosis (ORN)
- Shoulder dysfunction
- Taste changes
- Scarring